Could there be a reliable way to predict long-term health outcomes? Perhaps a specific food item, exposure to environmental factors like pollution or UV rays, or even a particular gene or DNA marker. For decades, countless researchers and policymakers pursued this question, searching tirelessly for a variable that could reliably predict health conditions. Such a discovery promised to revolutionize preventive public health.
Despite rigorous scientific efforts and millions of dollars in funding, the answer remained elusive—until 1998. That year marked a eureka moment for Dr. Vincent Felitti and Dr. Robert Anda. Through their groundbreaking research, they uncovered the missing piece: an elusive variable capable of predicting adult health risk behaviors, health status, and disease states.
The 1998 Adverse Childhood Experiences Study (ACE Study), conducted by physicians Dr. Felitti and Dr. Anda in collaboration with the Centers for Disease Control and Prevention (CDC) and Kaiser Permanente, was groundbreaking in its findings. It revealed that adverse childhood experiences (ACEs) were not only alarmingly common within the population but were also strongly linked to the development and prevalence of numerous health problems. For the first time, this large-scale study provided concrete evidence of the lasting impact of childhood trauma on physical health outcomes, reshaping how we understand the connection between early adversities and adult well-being.
What are ACEs
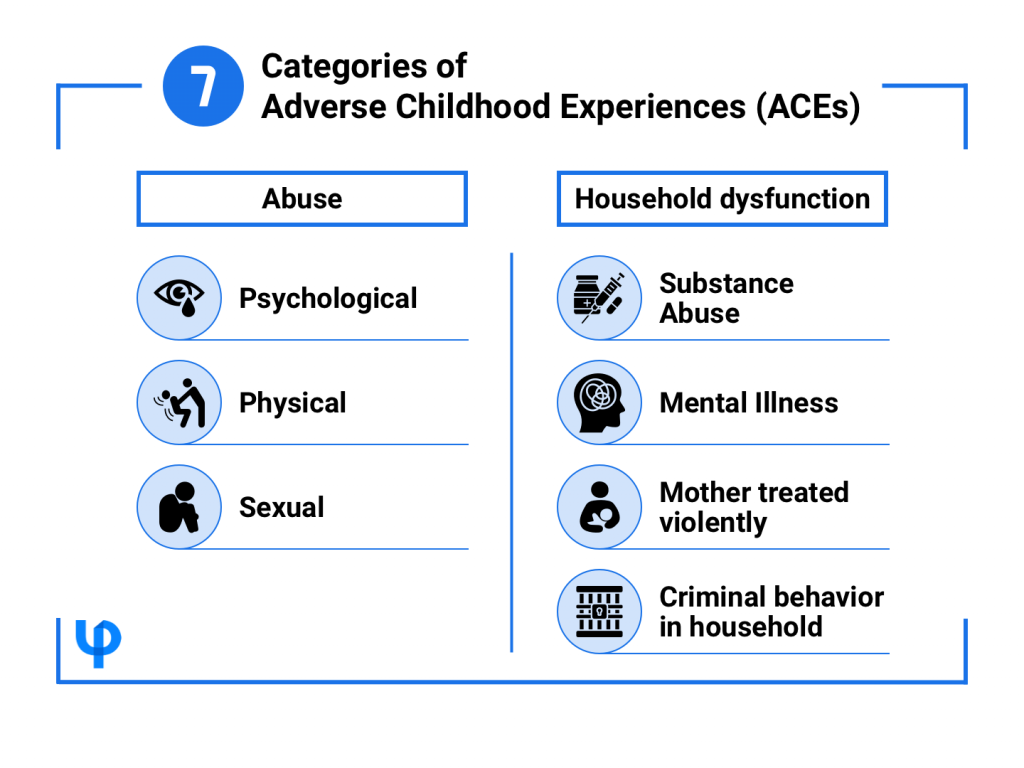
The term, “ACEs,” was coined in 1998 following the publication of the Adverse Childhood Experiences Study (ACE Study). Adverse Childhood Experiences (ACEs) are stressful or traumatic events experienced before age 18. They are grouped into three categories: abuse, neglect, and household dysfunction.
ACEs and Negative Health Outcomes
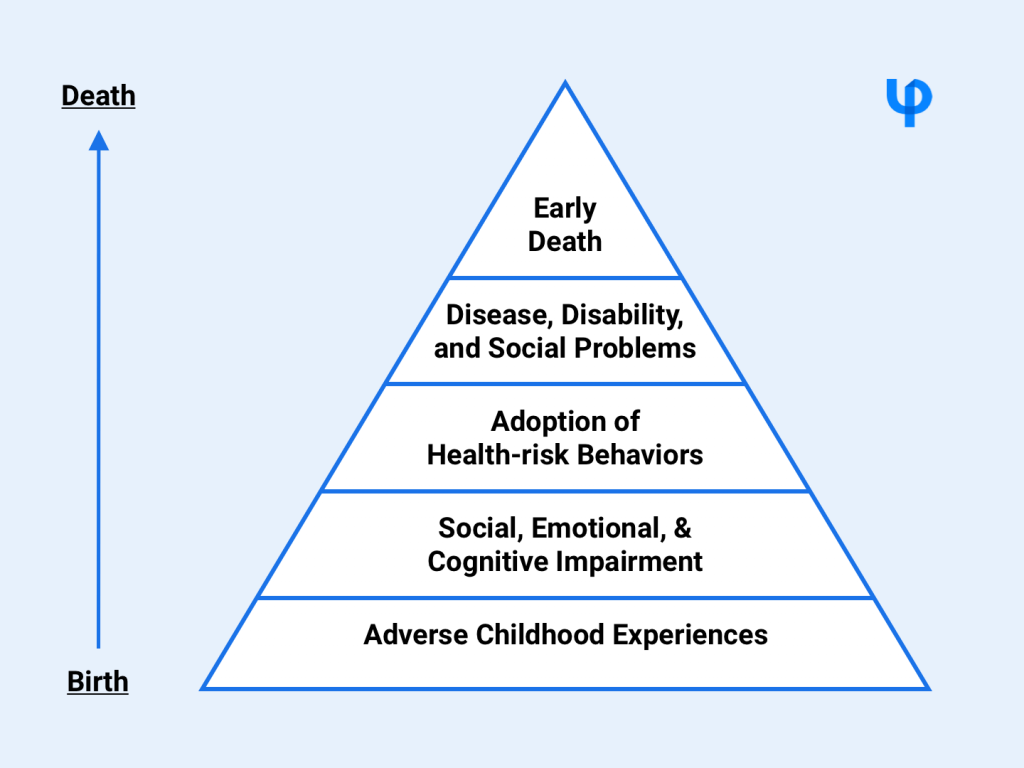
The ACEs study found a strong graded relationship between the breadth of exposure to abuse or household dysfunction during childhood and multiple risk factors for several of the leading causes of death in adults.
Persons who had experienced four or more categories of childhood exposure, compared to those who had experienced none, had:
- 4- to 12-fold increased health risks for alcoholism, drug abuse, depression, and suicide attempt;
- a 2- to 4-fold increase in smoking, poor self-rated health, ≥ 50 sexual intercourse partners, and sexually transmitted disease; and
- a 1.4- to 1.6-fold increase in physical inactivity and severe obesity.
The number of categories of adverse childhood exposures showed a graded relationship to the presence of adult diseases including ischemic heart disease, cancer, chronic lung disease, skeletal fractures, and liver disease. The seven categories of adverse childhood experiences were strongly interrelated and persons with multiple categories of childhood exposure were likely to have multiple health risk factors later in life.
Rationale for Screening ACEs
For behavioral health practitioners, screening for Adverse Childhood Experiences (ACEs) is a critical step in understanding the root causes of mental health challenges. ACEs are not only widespread but also deeply intertwined with conditions like depression, anxiety, PTSD, substance use disorders, and chronic health issues. Routine screening allows therapists and behavioral health clinics to adopt a trauma-informed approach, tailoring interventions that address both immediate symptoms and underlying trauma. While primary prevention efforts focus on reducing ACEs at a societal level, behavioral health professionals play a key role in secondary and tertiary prevention—helping clients recognize maladaptive coping mechanisms, develop healthier responses, and mitigate long-term health risks. Despite concerns that discussing ACEs may be distressing, research indicates that clients are receptive to these conversations, reinforcing the importance of integrating ACE screening into behavioral health assessments.
Screening Tools for ACEs
Screening for Adverse Childhood Experiences (ACEs) is an essential step in recognizing individuals at risk for long-term health challenges. Several standardized tools have been developed to assess ACE exposure across different age groups, helping behavioral health practitioners adopt a trauma-informed approach. These tools provide a structured way to identify adversity and guide appropriate interventions.
These tools are also available on PsyPack for digital administration and automatic scoring, making the assessment process more efficient for practitioners.
| Screening Tool | Target Age Group | Format | Number of items |
| Adverse Childhood Experiences Questionnaire (ACE-Q) | 18 years and above | Self-report questionnaire | 10 |
| CYW Adverse Childhood Experiences Questionnaire for Adolescents : Self Report (CYW ACE-Q Teen SR) | 13-19 years | Self-report questionnaire | 17 |
| CYW Adverse Childhood Experiences Questionnaire for Adolescents (CYW ACE-Q Teen) | 13-19 years | Parent/Caregiver-administered | 17 |
| CYW Adverse Childhood Experiences Questionnaire for Children (CYW ACE-Q Child) | 0-12 years | Parent/Caregiver-administered | 17 |
Using ACE Screening in Practice
Incorporating ACE screening into clinical practice can help behavioral health practitioners gain deeper insights into a client’s history and tailor interventions accordingly. ACE screening tools can be used during initial assessments to identify potential trauma-related risk factors, guide treatment planning, and inform trauma-informed care approaches. They can also support early intervention efforts, helping clinicians recognize patterns that may contribute to long-term health and behavioral challenges.
While screening alone does not diagnose trauma-related conditions, it serves as a valuable starting point for meaningful conversations between practitioners and clients. The results can help clients better understand their experiences while allowing clinicians to provide appropriate resources and interventions.
To streamline the screening process, digital platforms like PsyPack offer ACE screening tools with automatic scoring and report generation, making it easier for practitioners to integrate these assessments into their workflow efficiently.
Conclusion
The groundbreaking ACE Study not only shed light on the long-term impact of childhood adversity but also demonstrated its predictive power in understanding mental health challenges. By integrating ACE screening into behavioral health practices, therapists can uncover critical insights into their clients’ experiences, helping to tailor interventions and improve clinical outcomes. As our understanding of trauma deepens, leveraging ACE assessments in practice can be a valuable tool in fostering resilience and promoting long-term well-being.